Layman's Guide to Medical Equipment 5
Tongue Depressor

I use it when your tongue is too happy and you are talking too much.
posted by angry doc at
5:02 pm
|
6 Comments
![]()
Tongue Depressor
posted by angry doc at
5:02 pm
|
6 Comments
![]()
Pen Torch

posted by angry doc at
5:00 pm
|
13 Comments
![]()
angry doc was a little miffed at this advertisement when it first came out. 
Certainly in healthcare we all use a little bit of fear and scare-tactics to promote health, but it seemed to me putting the ad through the point of view (and in the TV commerical, the voice) of a little girl and guilt-tripping parents is a little bit of a low blow.
Nevertheless there is a message there and awareness should be raised, and so I did not rant about it.
The ST Forum today carries a letter from another doctor who is also unhappy with the ad, but for a different reason:
June 26, 2006
Don't reinforce prejudices by using disabled people to put across message
Public communication campaigns are meant to provide information, correct misperception, influence perception and attitude, and encourage responsible behaviour.
In using the mass media to do this, the communicator has to balance the message with the execution of the campaign.
In public health campaigns, using the fear factor is an effective way to drive home the message.
In a recent advertisement promoting pneumococcal vaccination for the young, a child in wheelchair was shown as a victim of non-vaccination.
The vaccination helps to protect against peneumococcal infections and thus can prevent the severe complications of the infection.
Though this public education campaign has a good intent, it is important to use evidence-based cause and effect link (like smoking being the most prevalent cause of lung cancer) to put across the message.
Otherwise, advertisements based on small variables can cause unnecessary and unfair generalisation and stigmatisation of disabled people.
The advertisement portrays a direct cause-and-effect slant, giving the impression that people become wheelchair users as a form of retribution for not doing something right.
This impression can reinforce the notion that people with disabilities are a burden to society and also wrongfully place the blame of a person's disability on him or his family for their inaction in preventing his disability.
In fact, over 90% of wheelchair and mobility aid users can be attributed to accidents, cerebral palsy, muscular disorders, diabetes, stroke, and ageing (frail elderly) rather than as a result of non-vaccination. The advertisement also portrays a very depressing and introverted view of disabled people.
The child on wheelchair was shown to be very inward and was unable to play or participate in any activities with the sister. This again reinforces the stereotypical perception that a person who is disabled is doomed and cannot engage actively in mainstream society.
In 2004, a survey commissioned by the National Council of Social Service revealed that people with disabilities were generally thought to be dependent and as having poor esteem, and that they didn't have opportunities to interact with the public.
The survey showed that 74% of the respondents remarked that people with disabilities had greater difficulties coping with day-to-day demands of life and 50% thought that disabled people could not have the same ambitions as able-bodied people.
This is not unexpected given that some advertisements persist to reinforce such unfair and wrong perception.
It is unfortunate that today, despite having the right motivation and appropriate devices, a disabled person could still be handicapped because the society and community make it so, by projecting untrue stereotypes and reinforcing social and physical inaccessibility.
There is really nothing to stop a child with disabilities from participating in mainstream activities. Wheelchair users can play tennis, basketball, modified hockey and football, and even sail. Like it or not, there is implicit prejudice in us, bias that emerges from our unconscious beliefs.
We learn to make associations, for example, old with grey hair, thunder with lighting, and so on. If we really aim at being an open and inclusive society, then efforts must be made to eliminate as much as possible these unnecessary prejudices in all our public communication.
Could the advertisement have achieved its intent without singling out disabled people? We believe so.
Dr Ow Chee Chung
Executive Director
Society for the Physically Disabled
angry doc is confused.
As far as he could make out from the advertisement, the boy is unable to play with his sister normally because he has had brain damage from meningitis. He certainly didn't get the idea that all disabled people are a burden to society and that they or their family are all to blame for their disabilities.
Is it unfair to depict a brain-damaged boy in a wheelchair as being unable to play with his sister?
Will it be acceptable to depict the same boy, NOT in a wheelchair (and WITHOUT any physical disability), as being unable to play normally with his sister?
Is it wrong to depict physically-disabled people as being unhappy?
The physically-disabled do face many barriers and many prejudices in our society, but angry doc doesn't really think that this advertisement, disagreeable as it is to him for an entirely different reason, reinforces prejudices against them. People get the impression that physically-disabled people have a hard time in our society because they see them having a hard time in our society, not from a TV commercial.
Leaving aside the fact that physical disability in some cases is indeed a cause-and-effect result of preventable complications of diseases (e.g. in stroke, diabetes, and some accidents, as mentioned by Dr Ow), angry doc thinks it will be very hard for people in the health promotion business to do their job if people suffering from any condition may not be portrayed as being unhappy.
Should anti-smoking campaigns not be allowed to depict the sufferings of lung-cancer patients, because lung cancers are not invariably caused by smoking, and that some people view the dying process and struggle against cancer a noble 'learning process' and not necessarily a tragedy?
Should anti-drunk-driving campaigns not be allowed to show the aftermath of traffic accidents, because most traffic accidents are not the results of drunk-driving?
Should safe-sex not be a focus of anti-AIDS campaigns, because not all HIV transmission is through sexual intercourse?
I am sure you can think of other examples where the disease is not caused solely by the behaviour we are trying to discourage, or where the disease is not 'guaranteed' preventable by the behaviour we are trying to promote.
Does that mean that we should not depict patients and victims as patients and victims, for fear of offending sensibilities of those who fall outside our target 'cause-and-effect' group?
Will the day come when we no longer dare to portray certain groups of people in a negative light, even when the context is accurate, appropriate, and fair, for fear of public backlash, or being seen as being politically-incorrect or insensitive?
Perhaps the ad is not the only party using fear as a tool here.
posted by angry doc at
5:39 pm
|
1 Comments
![]()
A reader asked me this in a comment on my previous post, and I thought it was a topic worth discussing:
Angrydoc, do you find yourself doing certain procedures and examinations just for the sake of satisfying the customer's pre-conceived expectation that the doctor should be checking this for me and that for me even when it isn't necessary?
Or like doing more is good and less is bad?
On the other hand, do you also find yourself doing less sometimes because the patient's pre-conceived expectation is that he should not have certain unpleasant procedures done on him?
Eg patient complains of constipation/abdominal problems and you don't complete the physical examination by looking at the groin for hernia or perform a digital rectal examination? Patients give me the "funny look" when I want to check their groins for hernia and perform DRE.
So which is better? Having a patient walk out the door with a happy smiling face because the doctor has done what he wanted? Or having a patient walk out the door thinking, "Basket the doctor sick or what want to see my down there and stick finger in my ass!"
I think in the former the possibility of lawsuits and complaints to SMC are actually lower!
The issue of patient expectations as to what constitutes necessary and unnecessary examination is an important one. Ideally a doctor should be able to manage a patient's expectations and educate him on whether and why an examination is required or not. In reality we all know that it can be difficult. Still, it's something a doctor should think about.
Over the years I have come to form some opinions over this issue, some of which have come from reading of the MPS Casebooks.
As usual when it comes to discussion of clinical situations, a lot depends on the specific patient and clinical condition, but in generally I would say more is better than less when it comes to clinical examination (laboratory and radiological and other investigations are another altogether...).
Say you are sitting in an orthopaedic clinic and this healthy young man who is seeing you for an ankle sprain asks you to check his blood pressure. Certainly there is no real indication to do so, but it will take only a minute of your time and you might (just might) pick up a case of secondary hypertension. I find it hard to say 'no' in cases like this one.
You might get a complaint if you refused to check his BP, even if his BP was perfectly normal. It's something a reasonable person (and perhaps doctor too?) would expect a doctor to check and a simple examination that takes little time and costs, and is non-invasive. (If he asked for his AFP to be checked even though he has no risk factor, then it would be a different situation altogether.) And if he did turn out to have hypertension and suffered real damage as a result of a delayed diagnosis because you didn't check his blood pressure for him, he might even succeed in a suit against you.
In the reverse scenario of a patient refusing an examination which I think is required, I make it quite clear that without the examination I consider the consultation incomplete and that due to that I may decide not prescribe a treatment. I usually offer the patient the option to see another doctor or to refer the patient to a relevant specialist, but I never 'just give medicine' without completing an consultation properly. Always offer an option and a follow-up or referral, but never force a patient to undergo an examination.
The possibility of missing important diagnoses if you prescribe treatment without a proper examination is always there. An 'ezcema' which you don't bother to look at before you prescribed some steroid cream might turn out to be a skin cancer. An 'irregular menses' for which you did not perform a vaginal examination before you prescribed the woman some hormones may turn out to be a cervical cancer. The possibility of a complaint to SMC or even a lawsuit in such cases is of course very real. If you looked and made a wrong diagnosis, it's a case of error in judgement. If you didn't even look, it is negligence.
Now even if the examination revealed benign conditions or produced a negative findings and the patient filed a complaint, I seriously doubt any court or the SMC will find you guilty, as long as you did not force or coerce the patient into the examination (in which case it becomes battery, if I have my law right).
It is true that patients tend to complain when they are unhappy (for whatever reason) rather than for real negligence or damages, so by not acceding to their request for or refusal of an examination you will be setting up yourself for more complaints. However, if your reasons for requesting or refusing to perform an examination are sound, then it is likely that these complaints will not stick. On the other hand, if you agree to not performing an examination when it is clinically indicated simply because the patient would rather you did not and you missed an important diagnosis, then the complaint when it comes may possibly end your career.
I'd rather be safe than popular.
posted by angry doc at
2:08 pm
|
9 Comments
![]()
Sphygmomanometer
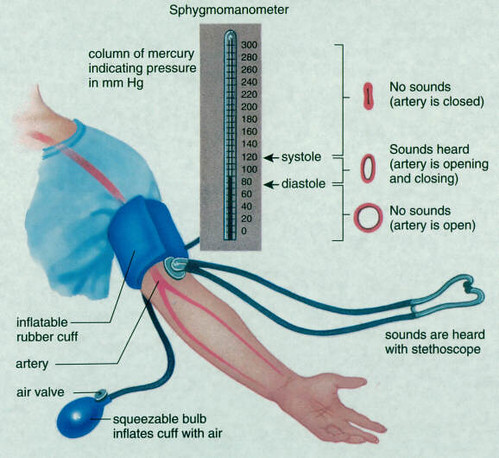
Nevermind how you pronounce it - it's the blood pressure thingy.
It measures your blood pressure by measuring the air pressure required to squeeze your arm blood vessel shut.
That's why we need to pump the cuff up with air.
That's also why you shouldn't ask me what your blood pressure is before I pump the cuff up.
It also does not measure your blood sugar or cholesterol levels - the cuff is not some sort of transdermal sensor.
posted by angry doc at
9:22 pm
|
2 Comments
![]()
Clinical Thermometer
This measures your body temperature.

and the one that goes inside your ear.

Try to remember which one is which, and offer the appropriate orifice when I hold out the thermometer.
Please.
I am embarrassed for the both of us.
posted by angry doc at
5:47 pm
|
5 Comments
![]()
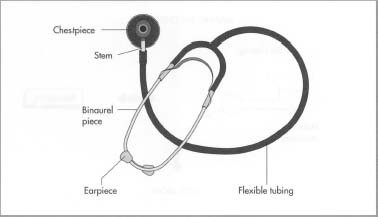
Stethoscope
posted by angry doc at
5:59 pm
|
5 Comments
![]()
K and I went for a talk on integrative medicine yesterday afternoon.
One of the speakers made angry doc's spidey sense tingle, and I googled up his name last night.
Here's one article 'for' him.
Here's one article 'against' him.
And here's an abstract of the study which was referred to in the talk and also the interview linked to above.
You decide.
Labels: alternative medicine
posted by angry doc at
8:16 am
|
1 Comments
![]()
Interesting letter from Dr Tan Min-Han in the ST Forum today.
June 16, 2006
How to keep Singapore health-care top-notch
IN THE two overview articles published in Review (ST, June 9), the Singapore health-care system came in for high praise. Few doubt that Singapore has a top-notch health-care system, allowing near-universal access to high-quality services.
Both articles alluded to, but did not expand upon, the forces for change in the Singapore health-care system.
While Singapore has developed a very successful health-care system over the last two decades, our changing environment demands equally nimble adaptation on our part. Upcoming challenges include an ageing population, steeply priced new technology and drugs, rising public expectations and the need to develop clinical research infrastructure to accompany investment in basic life sciences.
Even as we seek to maximise each dollar spent, our national expenditure on health is likely to continue its inexorable rise over the next few decades.
Today, novel drug regimens and surgical intervention can easily cost tens of thousands of dollars. It is no surprise that health-care costs are one of the main concerns of the man in the street.
With ever-increasing demands on national resources, a transparent and independent forum for technology and pharmaceutical appraisal is urgently required at the national level.
As cost-benefit ratios vary from society to society, Singapore must develop its own system for technology appraisal, possibly modelled after the National Institute of Clinical Excellence in Britain.
This forum should examine not just the clinical usefulness of a particular new drug, but also the societal benefits and costs in the local context from implementation.
For this to happen, substantial investments in health-policy research must occur, together with greater visibility of socioeconomic, financial and health-care data for accurate determination of societal outcomes.
Critically, an approach integrating both clinical and accounting principles will have the dual benefit of addressing both the supply and demand sides of expanding health-care costs, as organisations and the public are likely to respond to independent guidelines which are perceived as impartial.
As there is wide acceptance in Singapore of the premise of shared responsibility, this forum can be a basis for establishing degrees of co-payment for the pillars of our 3M health-care system: Medisave, MediShield and Medifund.
Non-governmental organisations such as charities will find this helpful in appropriate fund allocation and avoidance of wastage.
If truly worthwhile interventions can be distinguished from the over-hyped, funding and subsidy should be allocated correspondingly, ensuring that the dollars of the Government and the patients are well spent.
Dr Tan Min-Han
Dr Tan (if he is the same Dr Tan I am thinking of) is an intelligent person, and I used to enjoy reading his posts on an online forum. Heck, anyone who says 'drug regimens' instead of 'drug regimes' is in my good books.
He mentions the National Institute for Health and Clinical Excellence in his letter; I think I will be browsing through their site over the weekend.
Locally, a similar system in the form of MOH Clinical Practice Guidelines issued to all doctors has been in operation. But as Dr Tan noted, these guidelines do not yet go into cost-effectiveness in the context of our subsidised healthcare system.
Let's wait and see what the Ministry's response to his letter will be like.
Labels: letters
posted by angry doc at
5:33 pm
|
13 Comments
![]()
Sometimes I get a feeling that Help-line protocols are written just to piss callers off so the company doesn't actually need to give any help.
I just hope the obstructionist jerk who wrote the protocol I had to struggle through this morning doesn't end up getting a taste of his own medicine when he needs medical help, like in the scenario below:
Caller: Help! Someone just crashed his car into a tree – we need an ambulance here, quick!
Despatch: Sure. What is your name please?
Caller: My name's Caller. Please hurry!
Despatch: Good. How do you spell that?
Caller: Er… C-A-L-L-E-R.
Despatch: Good. May I have the model and the license-plate number of the car please?
Caller: What? Why do you need to know that? There’s a guy inside the car and he looks hurt – does it matter what make the car is?
Despatch: Mr Caller, we need to log the information before we can despatch an ambulance.
Caller: Er… OK… it's a Qia Meridian, and the license-plate is YI108N.
Despatch: Good. What colour is it, please?
Caller: What? What does that matter? There’s an injured man in a car - aren't you at all interested to know where this is?
Despatch: Sir, I’ve already told you – we need to log the information before we can despatch…
Caller: That's stupid!
Despatch: Sir, that’s our protocol, and as a matter of fact we are rather proud of our ISO certification. Now the colour, if you'd please.
Caller: Er… the car just burst into flames, so I guess it's sort of an orangey-red now. It'll probably be soot-black in a few more minutes but I can't be sure. Can you send a fire-engine round too?
Despatch: Sorry, you'll have to make another call at this same number for a fire-engine.
Caller: What? But I'm already on the line with you! Can't you just send a fire-engine too so I won't have to repeat all that useless information I just gave you?
Despatch: No, you'll have to make a separate call so we can assign you a separate service number.
Caller: Would you mind putting your ear-piece to your cheek? I would like to slap you through the phone-line.
posted by angry doc at
5:00 pm
|
4 Comments
![]()
The question of uptake rate of AMD was raised on a previous discussion, and the answer from the ministry has attracted this letter to the ST Forum:
June 5, 2006
Need for better way to sign advance medical directive
I READ with shock in the article on advance medical directives (AMDs) that the Advance Medical Directive Act was passed 10 years ago, yet only 3,840 Singaporeans have signed it ('A measure of control when the end comes'; ST, May 26).
I was first aware of the AMD when the Terri Schiavo case in the United States brought much publicity last year. My husband and I agreed we should both sign an AMD. Procrastination is the thief of time. However, we still haven't done it.
I am sure many Singaporeans feel the same as us but have delayed an AMD because it is inconvenient.
Look at the requirements.
First you must find a doctor who knows what the AMD is and is willing to act for you. It was reported that many doctors do not know how the AMD works. This is understandable.
Then you need a witness aged 21 or above.
Finally, consultation charges range from $10 to $30.
If not for the second requirement, we would have done it without hesitation. It is just unfair to impose something like this on a friend who knows also knows next to nothing about AMDs. Moreover, we will have to inconvenience the witness to go to the clinic to wait for the signing.
Besides, the witness may worry about what may happen in future should complications arise from the AMD.
To encourage more people to come forward and sign the AMD without delay, I would like to make a few suggestions.
First, have a team of doctors familiarised with explaining the AMD and form signing.
Second, have two doctors sign the form, one as the witness. If not, a doctor and a lawyer or someone appointed by the Government.
Third, as more people will be expected to sign when the requirements are made easier, why not arrange the signing at a specific place, for example a school, for a week initially and then on a certain day on a monthly basis?
Fourth, since a crowd can be expected, rather than doctors having to explain the AMD to every individual, why not have a doctor go on stage to explain to an 'audience' in front of the witness and have a mass signing after that? This will be more productive and can be repeated at hourly or two-hourly intervals. Recording and replaying a tape to the audience can also be considered if acceptable.
Finally, a standard charge can be imposed but should be kept low.
Won't this be better for us if we don't have to mingle with the sick in the clinic and add extra time to the queue when priority should be given to patients who need to be attended by the doctor?
We also need not give stress to friends by asking them to be our witnesses.
I hope the authorities will amend the requirements to facilitate signing of the AMD.
Emily Tai Kim Mooi (Mdm)
People who write to the ST Forum seem to be easily shocked or astonished.
Well, angry doc is shocked at Mdm Tai's proposal.
The signing of the AMD is and should remain a personal choice. I do not understand why Mdm Tai is so keen to 'encourage more people to come forward and sign the AMD without delay', or why she expects that crowds will rush to have AMDs signed if it was made more convenient.
As I said before I do witness AMDs, but I find the idea of a mass-signing a little creepy.
Call me old-fashioned, but I prefer to handle something as personal as a Living Will in a more personal manner. As I illustrated in a previous post, people have different understanding of the AMD and they may have different reasons for wanting to sign an AMD. It is important that the doctor who witnesses an AMD ensures that the patient understands its implications and that the doctor is convinced that the patient is not under duress to sign the AMD. It is a legal requirement, and for many doctors it will also be an ethical requirement on their part. You can't always do that in a single visit.
'Just listen to the recording and sign on the dotted line' isn't going to satisfy most doctors and patients, nor should it.
It isn't expensive to see a doctor. Really. And in the case of a Living Will there isn't really any rush. In fact, if there was any rush, your doctor probably shouldn't witness the AMD for you. In any case, having two doctors involved is not going to make it any cheaper, let alone throwing in a lawyer!
As for the need to for a second witness, the default is usually the clinic nurse (so much so that the ministry made a provision for the nurse to use the clinic address as 'her' address in the AMD), so this shouldn't be an issue in most cases.
Is getting an AMD signed inconvenient? Well, some letter-writers seem to have encountered difficulties getting an AMD witnessed.
Should it be made convenient? Well, it shouldn't be made inconvenient, and doctors who turn patients away should base their decision on their knowledge of the Act, the patient's personal circumstances and state of mind, and their own morals, and not ignorance of the Act. Patients who understand the implications of the AMD and are certain they want to sign one should be given access to a witness. Or witnesses.
But to turn it into a regular walk-in event where you make a decision involving a literally 'the rest of your life' issue after listening to a prepared speech or recording?
Well, if that is the alternative, then give me inconvenience anytime.
I for one certainly do not want to be the doctor sitting at one of these mass-signing sessions, witnessing AMDs for complete strangers, just so we can all be 'productive'.
If having an AMD is so important to you, then at least take some time and trouble to have it done properly. Please.
posted by angry doc at
11:50 am
|
5 Comments
![]()
posted by angry doc at
6:19 pm
|
0 Comments
![]()
angry doc will be taking a short break.
We hope to return to our regular ranting soon.
posted by angry doc at
5:05 pm
|
1 Comments
![]()
Bonus Bogus Story
China -
A leading automobile manufacturer in China is hoping to replace conventional seat-belts with 'qi-belts'.
Mr Zhuang Che, spokesman for Qia Motors revealed this to reporters in a news conference at the company's headquarters in Wuhan yesterday.
'Conventional seat-belts have been proven to save lives. However, they are made based on Newtonian physics. We are convinced that equally effective, if not better safety may be achieved using a system based on traditional Chinese philosophy,' said Mr Zhuang.
The novel system of qi-belts will be based on the ancient Chinese concept of qi, an invisible universal force.
'Qi cannot be measured using any instrument or device because modern science has yet to come up with something to measure it - that is the failure of modern science. However, the potency of qi has been demonstrated by practitioners all across the country. We have sufficient anecdotal accounts to conclude that it will offer adequate protection to passengers in the situation of vehicular collision. I am sure you have seen TV scenes of qigong masters having cars run over their abdomen without any apparent harm done to them, right?'
'Furthermore, conventional seat-belts are made of synthetic materials that seek to restrain the passenger. Qi-belts are all-natural and work on the more holistic principle of balancing the forces of motion and stillness when the vehicle meets an impact, so it's better for the passenger.'
According to Mr Zhuang, qigong masters working for the company will 'yun' or transfer their qi to car seats, thus imbuing them with the invisible force.
'All our qigong masters are certified by the National Qigong Council, which is made up of top qigong practitioners, so the quality of our qi-belt is assured.'
The qi-belt prototype will undergo field tests next month. The company is in the process of obtaining dummies for the crash-tests.
Labels: alternative medicine, bogus story
posted by angry doc at
8:32 am
|
4 Comments
![]()
This blog is not a substitute for medical advice. If in doubt consult your physician.

Works like no one's paying him, blogs like no one's reading, and hurts like he'll never be loved.









{kind=link}